Schizotypal Fact Sheet (version 2)
Schizotypal fact sheet version 2
Table of Contents
Symptoms
Ideas of reference
Magical thinking
Odd speech
Eccentricity
Social anxiety
No close friends
Unusual perceptual experiences
Constricted affect
Paranoid ideation
Common traits
Antagonomia
Delayed sleep phase
Ambivalence
Dyslexic-like traits
Motor control
Self disorders
Anomalous self experience
Hyper-reflectivity
Double bookkeeping
Childhood schizotypal personality disorder
The schizophrenia spectrum
Personality traits
Big Five
MBTI
Fisher temperament inventory
Attachment styles
Interests & Strengths
Cognitive ability and intelligence
Theory of mind
Relationship with worldviews and religiosity
Relationship with and differentiation from other disorders
Psychopathy
Borderline personality disorder
Schizoid, avoidant, paranoid, and schizophrenia
Bipolar disorder
Histrionic and narcissistic personality disorder
Obsessive-compulsive disorder and obsessive-compulsive personality disorder
Substance use
Mood disorders
Dissociative disorders
ADHD
Autism
Contrasting features of autism and schizotypal personality
Interests
Sexuality
Regulation
Social correlates
Worldviews
Cognition
Biological causes
Cannabinoid system
Serotonin system
Dynorphin system
Glutamate and NMDA receptors
Cognitive, psychological, and evolutionary causes
Predictive processing
Hyper-mentalizing
Imagination
Life history & sexual selection
Hyper-openness
Symptoms
Ideas of reference: A tendency to perceive and over-interpret social cues and social occurrences relating to one's self that are unlikely, and a tendency to over-mentalise (think about and detect others thoughts, intentions, and mental states) in relation to oneself [15].
Examples from schizotypy measures [13][14]:
“If I see someone laughing, I often wonder if they are laughing at me”
“I am not sure why, but people often seem to pay a lot of attention to me”
“Although I know deep down inside it is not true, I often feel that others blame me for things”
“I often wonder if radio DJs play songs just for me”
“People often fidget in their seats when I enter a room”
“When I see two people talking at work, I usually think they are criticizing me”
“I sometimes think that newspaper articles contain messages for me”
“People have been dropping hints for me”
“I spend time thinking about friends gossiping about me”
“I have been thinking a lot about people avoiding me”
“Even if they do not say it, it seems to me that other people are always wondering how smart I am”
Magical thinking: Persons with schizotypal personality disorder tend to experience passing magical thoughts and often have magical beliefs. Importantly, magical beliefs are only indicative of schizotypy if they are unconventional, not based on existing belief systems, and are self referential. This means that beliefs in christianity, witchcraft, astrology, etc are not the same as magical thinking and are not indicative of schizotypy, and persons with schizotypal personality disorder are actually much less likely to have conventional or pre existing belief systems than the general population [12].
Examples from schizotypy measures [16]:
“I have had the momentary feeling that someone’s place has been taken by a look-alike”
“At times I perform certain little rituals to ward off negative influences.”
“The hand motions that strangers make seem to influence me at times.”
“If reincarnation were true, it would explain some unusual experiences I have had”
“I have sometimes felt that strangers were reading my mind”
“I have had the momentary feeling that I might not be human.”
“Do you feel that your accidents are caused by mysterious forces?”
Odd speech: Persons with schizotypal personality disorder tend to have unusual patterns of speaking and may have difficulty articulating themselves properly.
Examples from schizotypy measures [17]:
“I use long, sophisticated and unusual words to say simple things”
“I notice that in conversations, I tend to go round in circles”
“I speak in whispers or mutter under breath for no obvious reason”
“It takes me an excessively long time to answer questions”
“I enjoy making up new words, which only have meaning for me”
“I find it hard to put into words what I want to say”
“I have only a ‘patchy’ memory of what has been said during a conversation”
Eccentricity: Persons with schizotypal personality disorder tend to be seen as odd and eccentric by others and have unusual behaviors. Importantly, this eccentricity is not the same as oddness caused by social deficits or autistic behaviors like strong interests in things that may be seen as “cringey” by others, atypical identities, or participation in alternative or fringe cultures.
Examples from schizotypy measures [19]:
“Considering my actions or speech, people tend to think that I’m pretty odd, eccentric, or weird.”
“Others have described my habits as unusual.”
“Other people see me as slightly eccentric”
Social anxiety: Excessive social anxiety often occurs in schizotypal personality disorder, and results in avoidance of social situations and interactions.
Examples from schizotypy measures [19]:
“Being around other people puts me on edge.”
“I often feel that I am making a bad impression on others”
“I'm really very awkward around people.”
“I often feel nervous when I'm in a group of unfamiliar people.”
“ I sometimes avoid going to places where there will be many people because I will get anxious.”
No close friends: Persons with schizotypal personality disorder tend to have little to no friends as a result of excessive social anxiety, paranoid fears, as well as a need for independence and detachment from commonly shared values, beliefs, and ways of thinking [18]. In schizophrenia, a lack of close friends may be increased additionally by anhedonia leading to social disinterest, however persons with schizotypal personality disorder typically do not experience true anhedonia or social disinterest [1], and tend to desire close relationships but are unable to fulfill their need for them [20][21], and generally only desire to form relationships with people who are "real" (that also question commonly shared values, beliefs, and ways of thinking) [18].
Unusual perceptual experiences: A tendency to experience fleeting, mild forms of hallucinations such as visual, auditory, tactile, and bodily distortions. Typically the person is aware that these distortions are hallucinations.
Examples from schizotypy measures [22][23]:
“When in the dark do you often see shapes and forms even though there is nothing there?”
“When you look in the mirror does your face sometimes seem quite different from usual?”
“Do you ever have a sense of vague danger or sudden dread for reasons that you do not understand?”
“I have felt that something outside my body was a part of my body.”
“I can remember when it seemed as though one of my limbs took on an unusual shape”
“Have you often mistaken objects or shadows for people or noises for voices?”
“Have you ever had the sense that some person or force is around you even though you cannot see anyone?”
“Do everyday things sometimes seem unusually large or small?”
Constricted affect: Persons with schizotypal personality disorder tend to have constricted and unusual expressions of emotion, especially socially. It is important to distinguish from social deficits where individuals might not understand or pick up on social cues, which is found in autism but not schizotypal personality disorder.
Examples from schizotypy measures [22]:
“People sometimes find me aloof and distant”
“I rarely laugh and smile”
“I am not good at expressing my true feelings by the way I talk and look”
“I tend to keep my feelings to myself”
Paranoid ideation: Persons with schizotypal personality disorder frequently experience paranoid thoughts and suspiciousness of others motives. Importantly, this is not the same as social cynicism, where the motives of others are seen as sinister and self serving - rather it tends to involve a preoccupation with being persecuted, excluded, conspired against, and typically occurs alongside ideas of reference [24]. It is also important to distinguish from political conspiracy theories which are often compared to paranoia, as these beliefs tend to be politically motivated, and not self-referential.
Examples from schizotypy measures [22][19][14]:
“I was convinced there was a conspiracy against me”
“People have been hostile towards me on purpose.”
“I often feel that there are hidden threats or put-downs in what people say or do.”
“I have to be on guard, even among people I know”
“I am sure I am being talked about behind my back”
“I think it's best not to let people know too much about you”
Common traits
Antagonomia: A characteristic of schizotypal personality disorder is a pervasive skepticism towards commonly shared belief systems, ways of thinking, assumptions, and values, and a choice to take an eccentric stance in opposition. Antagonomia is accompanied by the experience of being an "outsider" or "observer" of the social world which non-schizotypal individuals are embodied within, and drive to understand others in a detached, "morbid" intellectual, scientific-like manner and see what's "behind the curtains" [18][21]. Often individuals experience this as a gift, giving a sense of radical uniqueness and exceptionality of their being and their understanding of the world, which is referred to as "idionomia" [18]. It is thought that antagonomia in high functioning persons may lead to scientific creativity due to tendencies of questioning what is normally taken for granted [10].
Delayed sleep phase: "Night owl syndrome" was coined as a symptom of schizotypal personality disorder in one of the first criteria ever created for assessing schizotypal personality, describing a tendency for schizotypal individuals to sleep and wake much later than usual, and have high energy, clarity, and mood during the night but not during the day [77]. The modern term for this is "delayed sleep phase disorder".
Ambivalence: Persons with schizotypal personality disorder experience high levels of ambivalence, which refers to having multiple, contradictory thoughts and feelings toward something (e.g., love and hate) [78]. This includes thoughts and feelings about other people, one's self, and decisions.
Dyslexic-like traits: Schizophrenia spectrum disorders are strongly associated with traits of dyslexia and overlap in aspects of perception and language [104]. These may include trouble telling left from right, confusing the names of objects (e.g., saying table instead of chair), incorrectly remembering strings of text like phone numbers, frequently losing place and missing lines when reading, etc.
Motor control: Schizotypal personality disorder is associated with minor difficulties in motor control, and leads to difficulties with handwriting, using tools that require precision, etc. [79]
Self disorders
Anomalous self experience is considered to be a core feature of schizophrenia spectrum disorders, in that the self which is normally experienced ‘in the first person perspective as a self-present, single, temporally persistent, embodied, and bounded entity, who is the subject of his experiences’ [114] where ‘a stable sense of this basic selfhood and identity always goes together with an automatic, un-reflected immersion in the shared (social) world’ [114] and ‘the world is pre-given, i.e. always tacitly grasped as a real, taken-for-granted, self-evident background of all experiencing and all meaning’ [114] is disturbed, with a lack of core identity, profound alienation from the social world, and a diminished sense of embodiment, self presence, and “mineness” of internal experience. This is thought to lead to features of schizophrenia spectrum disorders including antagonomia, hyper-reflectivity, eccentricity, “double bookkeeping”, ambivalence, and social isolation [114]. Scales (examination of anomalous self/world experience) have been developed for assessing self disorders, and there are many different and specific manifestations of self disorders which are listed in these scales. There are too many items to list in this document, however the full list of items is available at Self-disorder - Wikipedia, and include anomalous experiences of space and time, language, embodiment, emotions, and existential orientation.
Hyper-reflectivity: Exaggerated self-consciousness and abnormally high levels of reflection and introspection, disengaging from typical involvement in society and nature, perceiving oneself from a sort of ‘third person perspective’ [114][115]. Hyper-reflexivity is conducive to increased understanding of how minds work with a tendency to analyze the minds of themselves and others, and high functioning schizophrenia spectrum patients often show interest in psychological science and psychoanalysis, with a higher frequency of schizophrenia spectrum traits in male therapists [116] (in other cases this often alternatively leads to interest in spiritual or political belief systems [114]). Carl Jung, a pioneer of personality psychology was highly introverted and had high levels of schizotypal traits and psychotic experiences [12]. Sigmund Freud’s personality was also suggestive of schizoid personality disorder, being described as aloof, disinterested in social events, hyper-reflective, and eccentric, known to have odd beliefs and struggling with substance abuse [117]. Friedrich Nietzsche, another early psychologist and philosopher also had strong indications of schizotypal traits and was highly introverted [118].
Double bookkeeping: A “split” experience of reality, where one reality is based in the laws of nature and independence of the mind from the external world, and the other reality is a private framework that violates the laws of nature, which co-exist [119]. Double bookkeeping is thought to explain non-empirical delusions (e.g., that one is destined to bring peace to humanity) which can occur while the patient is aware that the delusion is not real, as the private “delusional” reality and the physical, shared reality are unconnected [119].
Childhood schizotypal personality disorder
There is a common misconception that schizophrenia spectrum disorders begin at adolescence, however this is not the case, rather the onset of psychosis tends to occur in adolescence, but schizophrenia spectrum disorders and symptoms are present from childhood [80]. Children with schizotypal personality disorder have similar traits to adults with schizotypal personality disorder, and include oddness, abnormally severe social anxiety, abnormally high belief and investment in imaginary people, creatures, events, or worlds, ideas of reference, paranoid ideation, odd speech, attention problems and school difficulties, magical thinking, unusual perceptual experiences, unusual affect, social isolation, and unusually strong interests [79]. Childhood schizotypal personality disorder can be differentiated from autism in that children with schizotypal personality disorder show normal theory of mind abilities, and lack of autistic traits beyond social difficulties (e.g., sensory hypersensitivity, need for sameness) [80], differences between schizotypal personality disorder and autism become more clear into adulthood [81].
The schizophrenia spectrum
Like most mental disorders, schizotypal personality disorder is not a distinct category of personality and brain function, but is rather on a continuum with 'normal' personality, from no schizotypal traits all the way to severe schizophrenia [127]. Traits of schizotypal personality disorder in the general population are referred to as "schizotypy". Increased levels of schizotypy are characteristic of creative, imaginative, open-minded, eccentric individuals who may otherwise be high functioning and healthy [50][9]. The schizophrenia spectrum is also associated with the personality traits openness, introversion, and low conscientiousness [34][36]. Schizoid and avoidant personality disorder are schizophrenia spectrum disorders as of course are schizotypal personality disorder and schizophrenia [30].
Personality traits
Persons with schizotypal personality disorder tend to have high levels of openness to experience and neuroticism on the big five, as well as low conscientiousness and extraversion [1][4][5][34][36]. High openness to experience and low conscientiousness can distinguish schizotypal personality disorder from neurotypical controls as well as people with schizophrenia [1]. Schizophrenia spectrum disorders are genetically linked with high openness, neuroticism, and low conscientiousness [2][3]. Openness to experience relates to imagination, creativity, non-conformity, questioning of one's own morals and traditions, open-mindedness, reflectiveness, and high aesthetic sensitivity [123]. Conscientiousness relates to organization, tidiness, planfulness, responsibility, high sexual & moral disgust, high self restraint, low hedonism and sensation seeking, need for structure and routine, cautiousness, and conformity [38]. Extraversion relates to sociability, confidence, dominance, materialism, expressiveness, and status seeking [123][128][35].
In the MBTI model of personality, schizotypal personality is associated with introversion, intuition, thinking, and perceiving [6].
On the fisher temperament inventory, schizotypy is associated with lower cautious/social norm compliant temperament, higher prosocial/empathetic and curious/energetic temperament, and lower analytical/tough minded temperament [unreleased data].
Schizotypal personality disorder is associated with an anxious-avoidant attachment style [25].
Interests and Strengths
Schizotypal personality disorder, like many other psychiatric disorders like autism and bipolar disorder, is associated with a pattern of strengths and weaknesses as well as interests [11][12]. Persons with schizotypal personality disorder tend to have much more creative interests and hobbies than the general population such as music, entrepreneurship, poetry writing, photography, painting, comedy, and scientific research [7][8][9][10], and tend to have better cognitive abilities that are conducive to creativity, such as divergent thinking (i.e., thinking outside the box), associative thinking, global processing (“big picture” thinking), and imagination [9][11][12].
Cognitive ability & intelligence
A distinguishing characteristic of schizotypal personality disorder from schizophrenia is a lack of overall deficits in intellectual ability, and cognitive deficits in schizotypal personality mainly relate to attention and verbal learning [31]. Some evidence suggests that intelligence may affect the presentation of schizotypal personality disorder, with higher intelligence reducing the degree of magical thinking and paranormal belief as well as reduced social and sexual anhedonia, and leading to better overall function and more successful creativity, as well as better theory of mind ability and more accurate beliefs [98][99][100][101][102][103][12].
Theory of mind
Persons with schizotypal personality disorder have reduced cognitive empathetic ability and theory of mind on average, however evidence suggests that this is due to reduced cognitive ability that is associated with schizophrenia spectrum disorders, as well as differences in self experience and hyper-mentalizing, and positive schizotypal traits are positively associated with cognitive empathetic ability, though magical thinking specifically predicts reduced theory of mind [100][101][103][40][133][134][135][136][21][28]. Schizophrenia spectrum disorders are also genetically associated with high cognitive empathy [137], and persons with schizotypal personality disorder show the reverse pattern of brain activation in response to social stimuli in comparison to autism [138]. High functioning persons with schizophrenia spectrum personality disorders sometimes have particularly enhanced cognitive empathy [116]. Social dysfunction is associated with schizotypal personality disorder, however this social dysfunction is not caused by a deficit in cognitive empathy [21][28].
Relationship with worldviews and religiosity
It is sometimes thought that schizophrenia spectrum disorders increase religiosity, however there is only a grain of truth to this. Magical thinking and unusual experiences are conducive to religious and spiritual-like thinking (e.g., feeling the presence of a god, perception of mystical forces and intentionality in natural or innocuous events), however the relationship with schizotypy and religiosity is very weak and inconsistent, and is only found with positive schizotypy, with other aspects of schizotypy and overall schizotypy predicting lower religiosity, and typically only involve affective aspects of religiosity (e.g., search for meaning, feeling connected to a higher power, feeling at one with the world) [129][130][131][132]. Overall, evidence suggests that schizotypal personality disorder is negatively associated with religiosity and adherence to religious or spiritual belief systems, but is positively associated with unconventional spiritual beliefs and spiritual-like experiences, and are more likely to be “spiritual but not religious” [129][130][131][132]. Some measures of religiosity and spirituality are also conflated with aspects of dissociative and unusual perceptual experiences that do not necessarily measure religious or spiritual belief. Persons with schizotypal personality disorder tend to rely less on culture to form worldviews and update their worldviews more frequently than the general population, and are driven to question conventional values and ways of thinking [12][70][18] and these idiosyncratic worldviews may be religious or scientific in nature [12].
Relationships with other disorders
Psychopathy and Antisocial Personality Disorder
Psychopathy is a personality construct that consists of two components. Primary psychopathy refers to a component made up of callous, antagonistic behavior, a lack of empathy, dominant social behavior, manipulativeness, superficial charm and the ability to influence others, and high stress tolerance. Secondary psychopathy is made up of impulsivity, lack of planning, rebelliousness, hedonistic behavior (e.g., drug use, hypersexuality), rule breaking, and irresponsibility [26]. Antisocial personality disorder is a diagnosis that includes individuals who are high in either primary psychopathy or secondary psychopathy. Persons with schizotypal personality disorder have lower levels of primary psychopathy than the average person, however have much higher secondary psychopathy [26]. Impulsive non-conformity is considered to be a domain of schizotypal personality traits [23] and is nearly conceptually identical to secondary psychopathy. Persons with schizotypal personality are more likely to meet criteria for antisocial personality disorder as well as conduct disorder in childhood.
Borderline personality disorder
Schizotypal personality disorder and borderline personality disorder are highly overlapping, and most people with borderline personality disorder will have some schizotypal symptoms and vice versa [27][28]. Persons with borderline personality disorder however typically do not experience severe social anxiety, social isolation, extreme independence, and constricted affect however, which can differentiate schizotypal personality disorder from borderline personality disorder [29].
Other schizophrenia spectrum disorders
Schizotypal personality disorder exists on a spectrum with other schizophrenia spectrum disorders, which includes schizoid personality disorder, avoidant personality disorder, and schizophrenia [30]. Paranoid personality disorder is often thought to be on the schizophrenia spectrum, however paranoid personality disorder does not occur in schizophrenic relatives to the same extent as schizoid, avoidant, and schizotypal personality disorder, and may be more closely related to disorders characterized by antagonism such as narcissistic and antisocial personality disorder [30]. Avoidant personality disorder includes the schizotypal symptoms of excessive social anxiety and isolation, however does not include other symptoms. Schizoid personality disorder includes the social anxiety, isolation, independence, constricted affect, eccentricity, and odd speech symptoms of schizotypal personality disorder, however does not include other symptoms. Generally, people with schizotypal personality disorder will meet criteria for schizoid and avoidant personality disorder. Schizophrenia includes all of the symptoms of schizotypal personality disorder, however persons with schizophrenia experience severe and true hallucinations, high levels of anhedonia, and intellectual and social cognition deficits, and lower levels of openness and creativity, which can differentiate the two disorders [1][7][31].
Bipolar disorder
Bipolar disorder is very closely related to the schizophrenia spectrum, and it has been suggested that bipolar disorder may be on a continuum with schizotypal personality disorder and schizophrenia [32]. Most people with bipolar disorder will have symptoms of schizotypal personality disorder and vice versa [33].
Histrionic & Narcissistic personality disorder
Histrionic personality disorder is negatively associated with schizotypal personality disorder, particularly with negative symptoms [34], as histrionic personality disorder is characterized by high extraversion, as opposed to low extraversion which characterizes negative schizotypy [35][36]. Narcissistic personality disorder is also characterized by high extraversion, and is opposed to negative schizotypy [36], though superficial similarities between narcissism and schizotypy exist.
Obsessive-compulsive spectrum
The obsessive-compulsive spectrum consists of obsessive-compulsive disorder (OCD) and obsessive-compulsive personality disorder (OcPD). Schizotypal personality disorder and OCD are highly correlated with each other and overlap to some degree [37]. In contrast, schizotypal personality disorder is negatively associated with obsessive-compulsive personality disorder [34][36] which is characterized by high conscientiousness & low disinhibition [38], impulsive non-conformity being directly opposed to conscientiousness [36]. OcPD and schizotypy may appear to overlap in some aspects however this overlap is likely superficial and conflated with OCD.
Substance use
Persons with schizotypal personality disorder have a very high rate of substance use disorders compared to the general population, 67% of people meeting criteria for StPD having a diagnosable substance use disorder [39].
Mood disorders
Mood disorders including generalized anxiety, major depression, and panic disorder are very common in schizotypal personality disorder, as is the case in most psychiatric disorders [39].
Dissociative disorders
Persons with schizotypal personality disorder experience high levels of depersonalization and derealization, as well as a higher frequency of dissociative disorders [74]. It is thought that dissociation may be on a spectrum with schizotypy, and there is evidence for shared causes of psychotic experiences and dissociation [11][74][75].
ADHD
Symptoms of ADHD are very common in schizotypal personality disorder [75][76], and differences in attention and self regulation are thought to play a part in the causation of schizotypy [9][12].
Autism
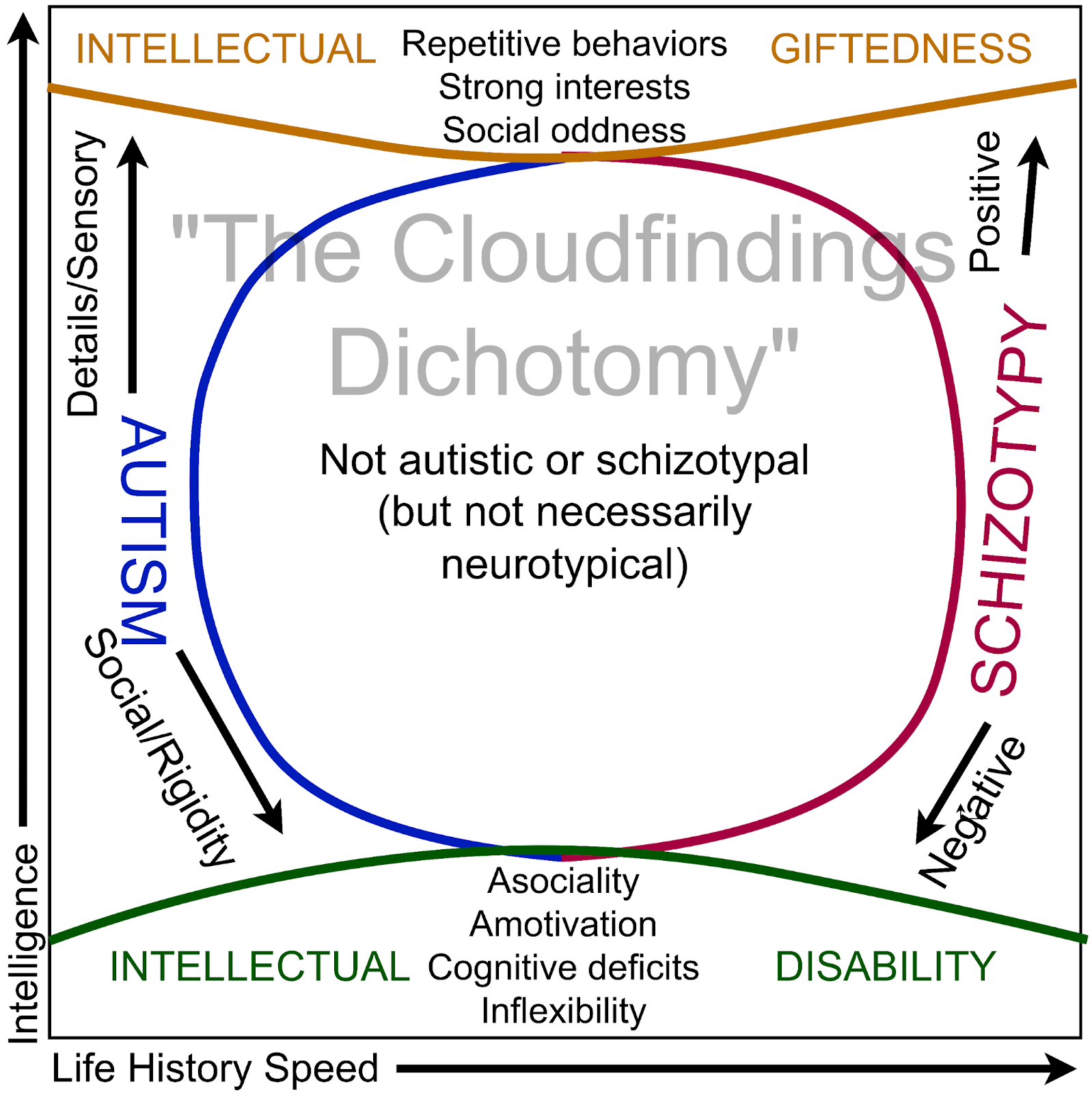
Autism and schizotypy may appear similar due to both disorders involving social difficulties, cognitive differences, high neuroticism, and other transdiagnostic symptoms that are found in many disorders (e.g., repetitive movements) [42][41]. However, careful, thorough, and theoretically informed examination of the relationship between autism and schizotypal personality disorder has shown that the two disorders are diametrically opposed in many aspects [43][32][12], and a negative relationship between autism and schizotypal personality emerges when conflating factors are controlled for [40][41]. Autism and schizotypal personality disorder are difficult to differentiate, and as of June 2023, there are no clinical tools that can adequately distinguish the two disorders, which leads to a high frequency of misdiagnosis and false comorbidity, however there is currently a self-report scale being developed to differentiate autism from schizotypal personality disorder, which is planned to be completed by the end of 2023 [44]. It is thought that autism and schizophrenia spectrum disorders can be comorbid, however true comorbidity (as opposed to two disorders being diagnosed due to superficial similarities between them) would either be characterized by severe intellectual disability or very high intellectual ability [105][106][107][108][109][110][111][112], and possibly would be characterized by childhood autism with schizotypal traits gradually increasing and autistic traits decreasing into adolescence and adulthood [113]. To aid in the distinction of the two disorders, a table of diametrically opposed traits of autism and schizotypal personality disorder is presented below.
Biological causes
Genetics and environment
Schizotypal personality disorder, like most mental disorders is largely genetic and exists on a continuum with normal personality traits like openness to experience which are also primarily genetic [83][2]. Childhood trauma may increase the severity of schizotypal symptoms, but are not sufficient to entirely cause schizotypal personality disorder [84].
Cannabinoid system
Cannabis is known to produce psychoactive effects which are similar to symptoms and correlates of schizotypal personality disorder, including paranoia, ideas of reference, visual/bodily/auditory distortions, increased imagination and creativity, increased aesthetic sensitivity, odd thinking, dissociation, and reduced motivation [82]. Persons with schizophrenia spectrum disorders have higher pain tolerance [96] and cannabis has pain relieving effects. Anandamide is a neurotransmitter produced naturally in humans that activates the same receptors as cannabis, and anandamide levels are increased in people with schizophrenia spectrum disorders [85]. Cannabis is also shown to temporarily worsen positive symptoms of schizophrenia spectrum disorders when administered [86].
Serotonin system
Activity in the serotonin system is associated with self regulation, conformity, conscientiousness, and low openness [87], which is the opposite pattern of traits associated with schizotypal personality disorder [1][2]. Persons with schizotypal personality disorder are found to have higher levels of the serotonin degrading enzyme monoamine oxidase [88], and lower expression of some serotonin receptors [32]. Serotonin also blocks dopamine release, meaning lower serotonin increases dopamine [89], and dopamine is associated with higher openness and positive schizotypal symptoms [89][90].
Dynorphin system
Dynorphin is a neurotransmitter which activates kappa-opioid receptors, and functions as a stress hormone that provokes attention to and avoidance of threats (anxiety), as well as analgesia and dissociation which protect against some of the deleterious effects of stress [91]. Agonists of kappa opioid receptors are found to cause psychotic-like symptoms including hallucinations, dissociation, paranoia, dysphoria, anhedonia, memory deficits, and delusions [91][92]. Dynorphin levels are associated with increased severity of schizophrenia spectrum disorders [93][94], though evidence of dynorphin abnormalities in schizophrenia spectrum disorders is somewhat inconsistent [95].
Glutamate and NMDA receptors
Glutamate is a type of excitatory neurotransmitter which activates NMDA receptors, along with other receptors. NMDA receptor blockers such as ketamine and dextromethorphan are shown to induce symptoms of schizotypal personality disorder, including sensory distortions, reduced sensory acuity, ideas of reference, paranoia, delusions, increased imagination and creativity, dissociation, reduced motivation, increased pain tolerance, odd behavior and thinking, and increased aesthetic sensitivity [97][85]. Persons with schizophrenia spectrum disorders are found to have lower levels of glutamate and NMDA receptors as well as higher levels of the neurotransmitter agmatine which blocks NMDA receptors [85].
Cognitive, psychological, and evolutionary causes
Predictive processing
Andersen (2022) put forth a model of schizotypy based on the predictive processing framework, where lower importance is attributed to sensory prediction errors for updating beliefs in individuals with high schizotypy [12]. Essentially, this means that schizotypy is a cognitive-perceptual specialization for processing chaotic and noisy data, where patterns and relationships exist but can only be detected if minor inconsistencies are ignored (i.e., focusing on the 'big picture'). Andersen suggests that a tradeoff exists in predictive processing, where giving higher weight to prediction errors prevents the detection of false patterns (i.e. apophenia) at the cost of being unable to detect higher level patterns (autism), and giving lower weight to prediction errors allows for the detection of higher level patterns at the cost of occasionally detecting patterns that don't exist, as in delusions and hallucinations that occur in schizotypy. This model explains features of schizotypy and previous models of schizotypy, such as the hyper-mentalizing model, hyper-associative cognition, the hyper-imagination model [11], antagonomia and idiosyncratic worldviews, attentional differences such as latent inhibition, hyper-openness, increased exploratory behavior, and enhanced cognitive abilities in insight problem solving, creativity, and global processing.
Hyper-mentalizing
The hyper-mentalizing model of schizophrenia spectrum disorders was originally put forth by Ahmad Abu-Akel [120] where it was suggested that theory of mind deficits in schizophrenia were caused by excessive mentalizing in contrast to deficient mentalizing in autism. This model has been elaborated on by several researchers, notably Bernard Crespi & Christopher Badcock who expanded the model to explain mental disorders beyond autism and schizophrenia, and have a basis in evolutionary theory, with a much larger and diverse body of evidence supporting the model [121]. Marco Del Giudice also expanded Crespi & Badcock's model, contrasting autism and schizotypy in terms of mating strategies and sexual selection, with a basis in life history theory and with relation to mental disorders beyond disorders explained by Crespi's model [32]. In this model, symptoms like ideas of reference, paranoia, erotomania, grandiose delusions, disorganized speech, and hallucinations (voices and people) are considered as exaggerated mentalizing, where they are all manifestations of excessive and dysregulated social cognition. Where in autism language is delayed and literal, persons with schizophrenia hallucinate speech, have disorganized speech, and over-interpret the meaning of speech to the point of paranoia. Autistic people have difficulty picking up social cues and reading emotions and thoughts, whereas in schizophrenia social cues in relation to oneself are perceived when they don't exist in ideas if reference. Autistic people pay less attention to and have difficulty picking up others intentions, whereas intent is perceived where it doesn't exist in paranoia and erotomania. This model is additionally supported by diametric correlates of the disorders, with social variables, neurobiology, cognitive abilities, development and behavior, emotionality, etc [121][85][43]. It is suggested by Crespi & Badcock that schizophrenia spectrum disorders are a dysfunctional byproduct of evolution, in contrast to some other models which view schizotypal personality as being selected for sexual fitness [46][122], though realistically it is likely that both are the case due to the heterogeneous nature of schizophrenia spectrum disorders [122].
Imagination
Bernard Crespi suggests that mentalizing is mostly underpinned by imagination, and that a hyper-developed imagination leads to hyper-mentalistic cognition, as well as dissociation, perceptual deficits, enhanced creativity, etc which occur in schizophrenia spectrum disorders, in contrast to autism which is associated with lower imagination [11]. This is supported by many lines of evidence such as imaginary companions in childhood being associated with higher schizotypy, artistic creativity and narrative generation being associated with schizotypy, and self reported imagination deficits being more strongly associated with reduced theory of mind than self-report scales of theory of mind [11][103].
Life history
Daniel Nettle originally put forth the hypothesis that schizotypal personality traits have been selected for due to schizotypy increasing traits that are beneficial to short term mating success [46]. Marco Del Giudice expanded this hypothesis with relation to life history theory and autism [50][41][122]. Studies have found that verbal and artistic creativity as well as non-conformity and cognitive empathy increase individuals desirability as short term mates and predicts having an increased amount of sexual partners [46][122][32]. In agreement with this hypothesis, schizotypal traits are associated with increased investment in short term mating, reduced investment in long term relationships, and more sexual partners [46][50][41][48] (expectedly, social anxiety and withdrawal correlate negatively with amount of sexual partners however, and the mating benefits of schizotypy are mainly in individuals with higher positive and impulsive schizotypy relative to disorganized and negative schizotypy, as well as intact intelligence [46][32]). Schizotypal personality also correlates highly with markers of a fast life history strategy, including impulsivity, sensation seeking, lower disgust sensitivity (excluding pathogen disgust), rebelliousness, disinhibition & disorganization, earlier maturation, lower socio-economic status and more traumatic environments, and detachment [32]. Schizotypal personality is positively associated with fast life history strategy disorders like borderline personality disorder, antisocial personality, ADHD, substance use, and bipolar disorder, and negatively with slow life history disorders like autism and obsessive compulsive personality disorder [32][40][34][73].
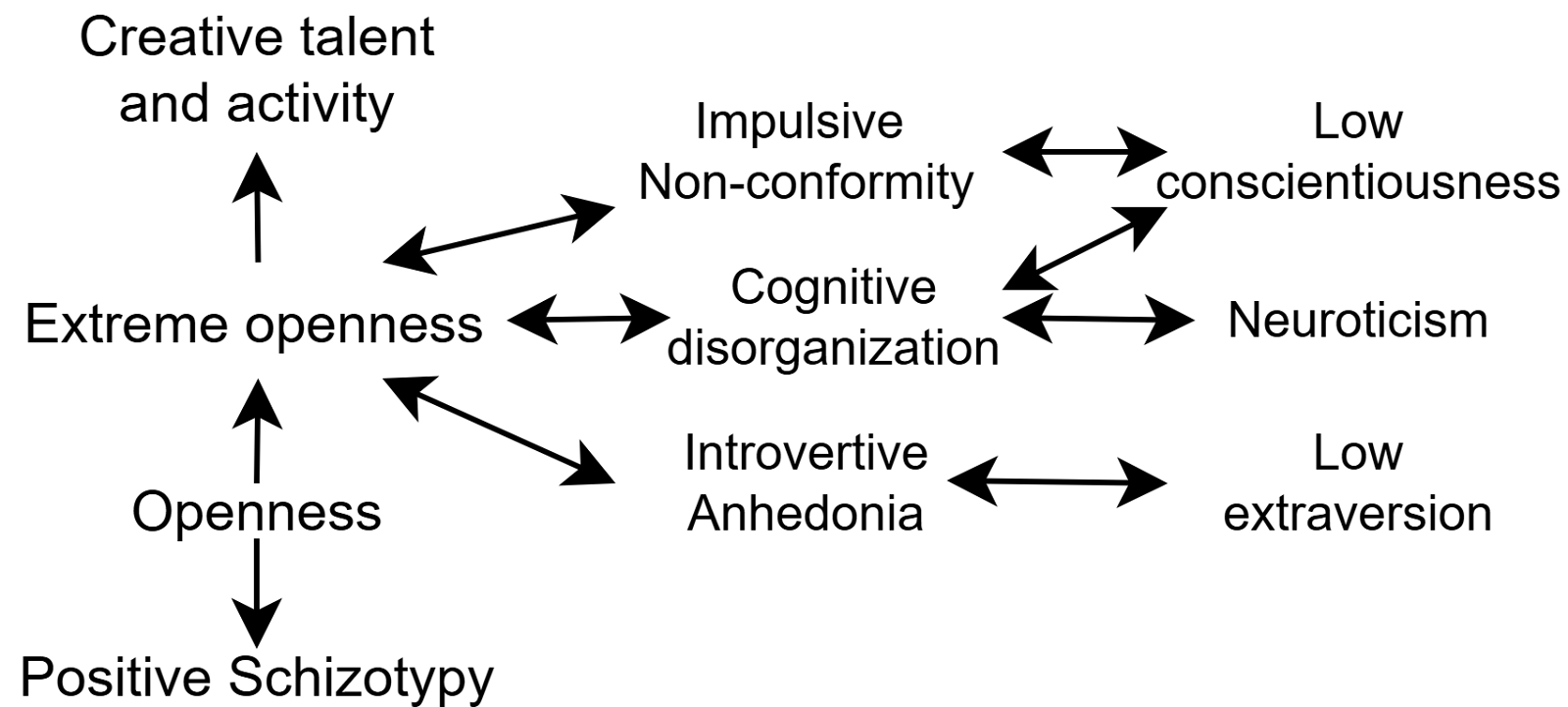
Hyper-openness & apophenia
Openness to experience is positively associated with intelligence and apophenia, however apophenia and intelligence are negatively correlated, suggesting a paradoxical nature of the trait. Schizotypy is also associated with openness and apophenia, but not intelligence. Colin DeYoung suggested that openness to experience is made up of two correlated traits, openness and intellect, and that an elevation of both traits leads to 'genius', but having too high openness relative to intellect leads to apophenia and schizotypy or 'madness' [123]. This is supported by findings such as magical thinking and paranormal belief being positively associated with openness but negatively with intelligence [123]. Several studies have confirmed that schizotypy maps well onto the trait openness to experience when separated from intelligence [123][124][125]. This model is quite similar to the imagination model of schizotypy, with imagination being conceptually similar to openness, and "imagination" has been used as an alternative name for openness to experience and is considered to be a facet of openness [126]. There is evidence that schizotypy may additionally relate to low conscientiousness and extraversion [1][2][5][34][36].
Camisa et al. (2005) Personality traits in schizophrenia and related personality disorders
Lo et al. (2017) Genome-wide analyses for personality traits identify six genomic loci and show correlations with psychiatric disorders
Smeland et al. (2017) Identification of genetic loci shared between schizophrenia and the Big Five personality traits
Couture et al. (2007) Personality characteristics and attachment in first episode psychosis: impact on social functioning
Gurrera et al. (2009) The five-factor model in schizotypal personality disorder
Segal (2001) An empirical investigation of Jung's psychological types and personality disorder features
Kinney et al. (2001) Creativity in Offspring of Schizophrenic and Control Parents: An Adoption Study
Karlsson (1970) Genetic association of giftedness and creativity with schizophrenia
Mohr & Claridge (2015) Schizotypy—Do Not Worry, It Is Not All Worrisome
Parnas et al. (2019) Schizophrenia and Bipolar Illness in the Relatives of University Scientists: An Epidemiological Report on the Creativity-Psychopathology Relationship
Crespi et al. (2016) Imagination in human social cognition, autism, and psychotic-affective conditions
Andersen (2022) Autistic-Like Traits and Positive Schizotypy as Diametric Specializations of the Predictive Mind
Lenzenweger et al. (1997) The Referential Thinking Scale as a Measure of Schizotypy: Scale Development and Initial Construct Validation
Freeman et al. (2021) The revised Green et al., Paranoid Thoughts Scale (R-GPTS): psychometric properties, severity ranges, and clinical cut-offs
Wastler & Lenzenweger (2019) Self-referential hypermentalization in schizotypy
Winterstein et al (2011) Brief assessment of schizotypy: Developing short forms of the Wisconsin Schizotypy Scales
Barrera et al. (2015) Formal Thought Disorder: Self-report in Non-clinical Populations
Stanghellini & Ballerini (2007) Values in persons with schizophrenia
Edmundson (2010) A five factor measure of schizotypal personality disorder
Martens (2010) Schizoid personality disorder linked to unbearable and inescapable loneliness
Stanghellini & Ballerini (2011) What is it like to be a person with Schizophrenia in the social world? A first-person perspective study on Schizophrenic Dissociality--part 2: methodological issues and empirical findings
Raine (1991) The SPQ: a scale for the assessment of schizotypal personality based on DSM-III-R criteria.
Mason et al. (2005) Short scales for measuring schizotypy
Pinkham et al. (2012) Qualitatively distinct factors contribute to elevated rates of paranoia in autism and schizophrenia
Berry et al. (2007) Attachment styles, earlier interpersonal relationships and schizotypy in a non-clinical sample
Ragsdale & Bedwell (2013) Relationships between dimensional factors of psychopathy and schizotypy
Zandersen & Parnas (2020) Exploring schizophrenia spectrum psychopathology in borderline personality disorder
Dinsdale et al. (2016) The ‘extreme female brain’: increased cognitive empathy as a dimension of psychopathology
Kwapil et al. (2022) Association of positive, negative, and disorganized schizotypy with cluster a, borderline, and avoidant personality disorders and traits
Wheeler (2013) Treatment of schizoid personality: an analytic psychotherapy handbook
Kirrane & Siever (2000) New perspectives on schizotypal personality disorder
Del Giudice (2018) Evolutionary Psychopathology: A Unified Approach
Kemp et al. (2018) Association of positive, negative, and disorganized schizotypy dimensions with affective symptoms and experiences
Kemp et al. (2022) Association of Multidimensional Schizotypy with PID-5 Domains and Facets
Ferguson & Negy (2014) Development of a brief screening questionnaire for histrionic personality symptoms
Cloudfindings (2023) General Psychopathology Masks the Associations Between Psychiatric Disorders and Personality Traits [retrieved from cloudfindingss.blogspot.com]
Brakoulias et al. (2014) The clinical characteristics of obsessive compulsive disorder associated with high levels of schizotypy
Samuel & Widiger (2011) Conscientiousness and obsessive-compulsive personality disorder.
Pulay et al. (2009) Prevalence, Correlates, Disability, and Comorbidity of DSM-IV Schizotypal Personality Disorder: Results From the Wave 2 National Epidemiologic Survey on Alcohol and Related Conditions
Nenadic et al. (2021) Subclinical schizotypal vs. autistic traits show overlapping and diametrically opposed facets in a non-clinical population
Del Giudice (2014) Autistic-like and schizotypal traits in a life history perspective: Diametrical associations with impulsivity, sensation seeking, and sociosexual behavior
Crespi (2020) How is quantification of social deficits useful for studying autism and schizophrenia?
Crespi & Go (2015) Diametrical diseases reflect evolutionary-genetic tradeoffs: evidence from psychiatry, neurology, rheumatology, oncology and immunology
Parvais et al. (2023) Protocol for the development and testing of the schiZotypy Autism Questionnaire (ZAQ) in adults: a new screening tool to discriminate autism spectrum disorder from schizotypal disorder
Andersen et al. (2022) Predictive processing and relevance realization: exploring convergent solutions to the frame problem
Cloudfindings (2022) Characterizing Repetitive Behaviors & Interests Specific to Autism: The Autistic Interests Scale [retrieved from cloudfindingss.blogspot.com]
Yang et al. (2022) Why iPlay: The Relationships of Autistic and Schizotypal Traits With Patterns of Video Game Use
Jonason et al. (2018) Love, Sex, and Personality Pathology: A Life History View of Personality Pathologies and Sociosexuality
Nettle & Clegg (2006) Schizotypy, creativity and mating success in humans
Del Giudice (2010) The evolution of autistic-like and schizotypal traits: a sexual selection hypothesis
Watts et al. (2017) Personality Disorder Features And Paraphilic Interests Among Undergraduates: Differential Relations And Potential Antecedents
Whitehouse et al. (2011) Brief report: autistic-like traits in childhood predict later age at menarche in girls
Ingudomnukul et al. (2007) Elevated rates of testosterone-related disorders in women with autism spectrum conditions
Ekblad (2018) Asexuality: A possible background and how it relates to autism and neurodiversity
Strunz et al. (2016) Romantic Relationships and Relationship Satisfaction Among Adults With Asperger Syndrome and High-Functioning Autism
Wainer et al. (2011) The structure and nature of the broader autism phenotype in a non-clinical sample
Bejerot & Eriksson (2014) Sexuality and Gender Role in Autism Spectrum Disorder: A Case Control Study
Pecora et al. (2019) Characterising the Sexuality and Sexual Experiences of Autistic Females
George & Stokes (2018) Sexual Orientation in Autism Spectrum Disorder
Anckarsater et al. (2006)The Impact of ADHD and Autism Spectrum Disorders on Temperament, Character, and Personality Development
Yule et al. (2021) Decreased risk for substance use disorders in individuals with high-functioning autism spectrum disorder
Weir et al. (2021) Understanding the substance use of autistic adolescents and adults: a mixed-methods approach
Russel et al. (2019) Mapping the Autistic Advantage from the Accounts of Adults Diagnosed with Autism: A Qualitative Study.
Werner et al. (2007) Socioeconomic status at birth is associated with risk of schizophrenia: population-based multilevel study.
Durkin et al. (2010) Socioeconomic inequality in the prevalence of autism spectrum disorder: evidence from a U.S. cross-sectional study.
Leonard et al. (2011) Autism and intellectual disability are differentially related to sociodemographic background at birth
Overskeid (2016) Power and autistic traits
Campbell et al. (2012) Familial linkage between neuropsychiatric disorders and intellectual interests.
Wheelwright & Baron-Cohen (2001) The link between autism and skills such as engineering, maths, physics and computing: a reply to Jarrold and Routh
Cloudfindings (2023) Moral Absolutism as a Theory of Mind Deficit [retrieved from cloudfindingss.blogspot.com]
Cloudfindings (2021) Literal Language Scale: Development & Association With Social Intelligence [retrieved from cloudfindingss.blogspot.com]
Butwicka et al. (2017) Increased Risk for Substance Use-Related Problems in Autism Spectrum Disorders: A Population-Based Cohort Study
Cloudfindings (2022) Obsessive Compulsive Personality Disorder as an Autism Spectrum Disorder [retrieved from cloudfindingss.blogspot.com]
Simeon & Hamilton (2008) Depersonalization disorder and schizotypal personality disorder
Cicero & Kerns (2010) Can disorganized and positive schizotypy be discriminated from dissociation?
Ettinger et al. (2006) Schizotypy, attention deficit hyperactivity disorder, and dopamine genes
Meehl (1964) Manual for use with Checklist of Schizotypic Signs
Deters et al. (2022) The Schizotypal Ambivalence Scale: An Item Response Theory Analysis
Jones et al. (2014) The Melbourne Assessment of Schizotypy in Kids: A Useful Measure of Childhood Schizotypal Personality Disorder
Tonge et al. (2020) Schizotypal Disorder in Children—A Neglected Diagnosis
Esterberg et al. (2013) Prodromal and Autistic Symptoms in Schizotypal Personality Disorder and 22q11.2 Deletion Syndrome
PsychonautWiki (retrieved 2023) Cannabis
Linney et al. (2003) A quantitative genetic analysis of schizotypal personality traits
Toutountzidis et al. (2022) Childhood trauma and schizotypy in non-clinical samples: A systematic review and meta-analysis
Crespi (2019) Comparative psychopharmacology of autism and psychotic-affective disorders suggests new targets for treatment
D'Souza et al. (2009) Cannabis and psychosis/schizophrenia: human studies
Fisher et al. (2015) Four broad temperament dimensions: description, convergent validation correlations, and comparison with the Big Five
Rogeness et al. (1985) Comparison of whole blood serotonin and platelet MAO in children with schizophrenia and major depressive disorder
Kapur & Remington (1996) Serotonin-dopamine interaction and its relevance to schizophrenia
DeYoung (2013) The neuromodulator of exploration: A unifying theory of the role of dopamine in personality
Leconte et al. (2022) Traumatic Stress-Induced Vulnerability to Addiction: Critical Role of the Dynorphin/Kappa Opioid Receptor System
Gonzales et al. (2006) Pattern of use and subjective effects of Salvia divinorum among recreational users
Lindstrom (1996) Clinical and biological markers for outcome in schizophrenia: a review of a longitudinal follow-up study in Uppsala schizophrenia research project
Moustafa et al. (2020) The endogenous opioid system in schizophrenia and treatment resistant schizophrenia: increased plasma endomorphin 2, and κ and μ opioid receptors are associated with interleukin-6
Shekhar (2019) Role of Kappa Opioid Receptors in Symptoms of Schizophrenia: What is the Neurobiology?
Stubbs et al. (2015) Decreased pain sensitivity among people with schizophrenia: a meta-analysis of experimental pain induction studies
PsychonautWiki (retrieved 2023) Dextromethorphan
Rizeq et al. (2020) An examination of the underlying dimensional structure of three domains of contaminated mindware: paranormal beliefs, conspiracy beliefs, and anti-science attitudes
Bronstein et al. (2019) Belief in fake news is associated with delusionality, dogmatism, religious fundamentalism, and reduced analytic thinking
Hughes et al. (2002) Longitudinal study of symptoms and cognitive function in chronic schizophrenia
Konstantakopoulos et al. (2014) Self-rated and performance-based empathy in schizophrenia: The impact of cognitive deficits
Polner et al. (2018) Insomnia and intellect mask the positive link between schizotypal traits and creativity
Nahal et al. (2021) Cognitive empathy as imagination: Evidence from reading the mind in the eyes in autism and schizotypy
Condray (2005) Language disorder in schizophrenia as a developmental learning disorder
Crespi (2008) Genomic imprinting in the development and evolution of psychotic spectrum conditions
Vaskinn & Abu-Akel (2019) The interactive effect of autism and psychosis severity on theory of mind and functioning in schizophrenia.
Abu-Akel et al. (2015) Perspective-taking abilities in the balance between autism tendencies and psychosis proneness
Bechi et al. (2022) Theory of mind and stereotypic behavior promote daily functioning in patients with schizophrenia
Bechi et al. (2021) Functional benefits of co-occurring autistic symptoms in schizophrenia is delimited by symptom severity
Kuszewski (2001) The Genetics of Creativity: A Serendipitous Assemblage of Madness
Crespi (2016) Autism As a Disorder of High Intelligence
Abu-Akel et al. (2020) Autistic and positive schizotypal traits respectively predict better convergent and divergent thinking performance
Crespi (2011) One hundred years of insanity: genomic, psychological, and evolutionary models of autism in relation to schizophrenia
Parnas (2012) The core gestalt of schizophrenia
Perez-Alvarez (2008) Hyperreflexivity as a condition of mental disorder: a clinical and historical perspective
McWilliams (2006) Some Thoughts About Schizoid Dynamics
Odajnyk (2012) Sigmund Freud: Introverted Spirited Power Physis Type
Cybulska (2019) Nietzsche: Bipolar Disorder and Creativity
Failla et al. (2020) Increased pain sensitivity and pain-related anxiety in individuals with autism
Abu-Akel (1999) Impaired theory of mind in schizophrenia
Crespi & Badcock (2008) Psychosis and Autism as Diametrical Disorders of the Social Brain
Del Giudice (2017) Mating, sexual selection, and the evolution of schizophrenia
DeYoung et al. (2012) From madness to genius: The Openness/Intellect trait domain as a paradoxical simplex
Bucher & Samuel (2021) Mapping a hierarchical dimensional structure of high experiential permeability: A bass-ackward approach to linking positive schizotypy and openness to experience.
Blain et al. Apophenia as the disposition to false positives: A unifying framework for openness and psychoticism
Sassenberg et al. (2023) Imagination as a facet of Openness/Intellect: A new scale differentiating experiential simulation and conceptual innovation
Magarotto et al. (2022) Moderately Eccentric: Evidence for Dimensionality in the Latent Structure of Schizotypal Personality Features
Highhouse et al. (2016) Status seeking and manipulative Self‐presentation
Hanel et al. (2019) Centrality of religiosity, schizotypy, and human values: The impact of religious affiliation
Crespi et al. (2019) Spirituality, dimensional autism, and schizotypal traits: The search for meaning
Carvalho et al. (2020) Relationship between religiosity domains and traits from borderline and schizotypal personality disorders in a Brazilian community sample
Willard & Norenzayan (2017) ‘‘Spiritual but not religious”: Cognition, schizotypy, and conversion in alternative beliefs
Bedwell et al. (2014) Latent factor modeling of four schizotypy dimensions with theory of mind and empathy
Yang et al. (2020) Exploring the links between alexithymia, empathy and schizotypy in college students using network analysis
Zhang et al. (2019) Network analysis of schizotypal personality traits and their association with other subclinical psychiatric features
Zhou et al. (2019) Revisiting the overlap between autistic and schizotypal traits in the non-clinical population using meta-analysis and network analysis
Warrier et al. (2018) Genome-wide analyses of self-reported empathy: correlations with autism, schizophrenia, and anorexia nervosa
Stanfield et al. (2017) Dissociation of brain activation in autism and schizotypal personality disorder during social judgments
Comments
Post a Comment